





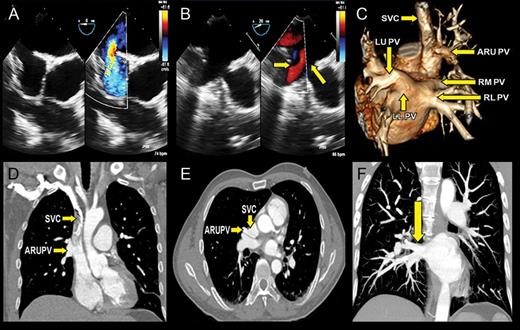
A 41-year-old man evaluated for recurrent blackouts was found to have dilated right heart chambers with signs of right ventricular volume overload. There were no valvular abnormalities, intracardiac shunts, or left-sided heart disease noted with transthoracic echocardiography. Transoesophageal echocardiography (TEE) confirmed a sinus venosus atrial septal defect (ASD) (Panel A) associated with four pulmonary veins draining into the left atrium (LA). The right superior pulmonary vein was visualized entering the LA adjacent to the sinus venosus ASD (Panel B). An abnormal vessel was draining blood into the superior vena cava (SVC) just above its entry into the right atrium (see Supplementary material online, Video S1). A 128-slice computed tomography scan confirmed four pulmonary veins draining into the LA (Panel C, arrows) as well as an anomalous right upper pulmonary vein (ARUPV) (Panels C–E, arrow) draining into the posterolateral aspect of the SVC. Computed tomography depicted the entire right middle lobe of the lung draining into what appeared to be the right superior pulmonary vein on TEE (Panel F). These findings were confirmed during surgery where the ARUPV was redirected via a baffle through the ASD.
This case highlights the importance of using complementary multimodality imaging to identify variations in pulmonary venous drainage that cannot always be accurately evaluated using TEE. In addition, it allows for accurate preoperative planning. LLPV, left lower pulmonary vein; LUPV, left upper pulmonary vein; RLPV, right lower pulmonary vein; RMPV, right middle lobe pulmonary vein.
Supplementary data are available at European Heart Journal – Cardiovascular Imaging online.

{kind=link}